
Leah Abrams

In the United States, rural residents do not live as long as their urban counterparts. This disparity has been widening for decades. Around 1970, urban life expectancy was 70.9 years, compared with 70.5 in rural areas, but by 2005–2009, the difference was greater (78.8 versus 76.8 years). In our research recently published in the IJE, we found that the gap in life expectancy would be even wider today if declines in cardiovascular disease (CVD) mortality had not dramatically slowed around 2010.
CVD, which includes all forms of heart disease, heart failure, atherosclerosis and hypertension, is the leading cause of death in the US. Its mortality rate had been rapidly declining for decades, thanks to reduced smoking, better hypertension control and use of statins, thrombolysis and stents. However, around 2010, this decline stagnated.
At the same time, improvements in national life expectancy stalled. In prior research, we showed that CVD mortality stagnation is the main culprit, even more so than recent increases in drug overdose deaths. However, little was known about the role of CVD mortality trends in recent rural–urban life expectancy differences.
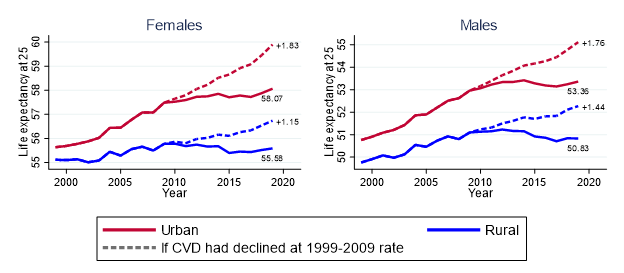
Using Centers for Disease Control and Prevention data on all 51,998,560 deaths in the US during 1999–2019, we first compared, over time, rural and urban life expectancy at age 25. We found that, from 1999 to 2009, the gap between urban and rural counties grew. Urban life expectancy increased 1.19 years more in women and 0.86 more in men compared with rural life expectancy. More recently (2010–2019), when overall US life expectancy stalled, rural counties experienced declines in life expectancy (–0.20 years for women and –0.30 years for men), while urban counties saw modest increases (0.55 years for women and 0.29 years for men). The rural–urban gap continued to grow during 2010–2019, but its pace was slower than in 1999–2009.
What would rural and urban life expectancies have been if CVD mortality had continued its decline rather than stagnating? To find out, we estimated life expectancies at age 25 under hypothetical conditions. This showed that, if CVD mortality had not stagnated, rural life expectancy during 2010–2019 would have increased by 1.15 years in women and 1.44 years in men, compared with the real changes. This suggests that CVD mortality stagnation was a main driver of the post-2010 decline in rural life expectancy. The effect on urban life expectancy was even greater (1.83 years in women and 1.76 years in men). CVD mortality stagnation’s impact on life expectancy is almost as large as the effect of the COVID-19 pandemic – 1.87 years. Overall, if CVD mortality had continued to decline at its pre-2010 pace, the rural–urban life expectancy gap would be even greater than it is now.
Interestingly, much of the effect of CVD mortality stagnation on life expectancy in both urban and rural areas is attributable to slowing improvements in mortality among adults aged over 65 years. This is surprising because overall life expectancy is influenced more by deaths at younger ages, and there is growing concern about increased mortality in midlife. However, so many CVD deaths occur in old age that slowing mortality declines in this group are a driving force of overall life expectancy trends.
A continued decline of CVD mortality across the US, especially in older adults, will be essential to improve life expectancy. Because the rural–urban gap was growing quickly while CVD mortality was robustly declining, efforts to rejuvenate that decline are not likely to reduce this difference unless an emphasis is placed on rural health. Evidence suggests that sustained community-wide programs targeting CVD risk factors like hypertension and hyperlipidemia, as well as behavioural changes like smoking cessation and increased physical activity, can effectively reduce rural CVD mortality. For widespread and sustained improvements in cardiovascular health and life expectancy, it will also be important to address more upstream factors that shape poor health in rural areas, such as static incomes, food insecurity and low levels of health care access.
Read more:
Abrams LR, Myrskyla M, Mehta NK. The growing rural–urban divide in US life expectancy: contribution of cardiovascular disease and other major causes of death. Int J Epidemiol 2021; 11 August. doi: 10.1093/ije/dyab158.
Leah R Abrams, PhD, MPH, is a Sloan Postdoctoral Fellow at the Harvard Center for Population and Development Studies. Her research pertains to equity in ageing, work/retirement, mental health and mortality. Twitter: @LeahRAbrams

This article sheds much-needed light on the rural-urban life expectancy gap, imparting precious insights into the effects of cardiovascular disease. Thank you for elevating attention to this essential issue.
LikeLike